Non-surgical Rehabilitation
The physical therapists at STAR Physical Therapy will help you recover through treatments designed to reduce pain and inflammation and, whenever possible, address the underlying problems causing your shin splints. The length of the physical therapy program varies for each patient, but as a guideline, you might expect to devote four to six weeks to your recovery and rehabilitation.
Reducing Inflammation
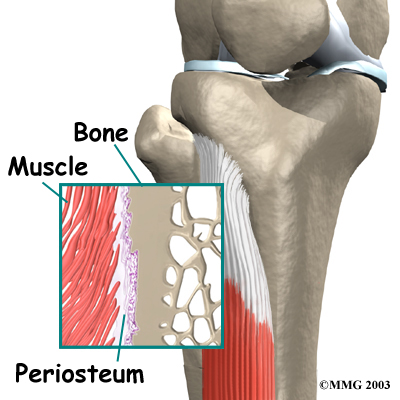
The purpose of your initial treatments at STAR Physical Therapy will be to reduce inflammation. Some of our patients suffering from shin splints receive iontophoresis, a technique where a mild electrical current is used to push a topical steroid medicine into the sore area. Ultrasound treatments, often used in combination with topical steroids, are also effective in halting pain and inflammation. To speed your recovery, our physical therapists may also use deep tissue massage along the junction where the sore tibialis muscle meets the tibia, followed by gentle stretching of the calf and tibialis muscles.
Our physical therapists will show you how to properly ice, rest, and if necessary, tape the injured area. Special taping techniques may be used to support the sore tissues and ease pain. However, we recommend that taping be used to help the area heal, not as a way to keep on training.
Foot Support
Your STAR Physical Therapy specialist will evaluate your posture and alignment to see if you have problems with pronation (arch flattening), a condition that we commonly see associated with posterior shin splints. Sometimes a small heel wedge, placed under the inside edge of the heel, is enough to ease tension on the posterior tibialis muscle. For more severe problems of pronation, we may recommend foot orthotics to support the arch and reduce stresses on the posterior tibialis muscle.
Rest and Recovery
During your recovery, stop doing the activity that caused the problem and avoid heavy training and sports activity for three to four weeks, or at least until the symptoms are under control. Rest and the application of cold packs play a key role in decreasing pain and inflammation in the early stages of treatment. Only after the pain starts to go away, should you begin to resume your normal routine.
Resuming Activity
As your pain starts to go away and you begin doing more normal activities, we will help you develop a recovery program to avoid overuse while training. This may include evaluating your running style, and suggesting tips on footwear and the use of shock-absorbing insoles. Knowing your training schedule, pace, and the surface you use can guide us in making personal recommendations as you attempt to safely resume your sport.
Post-surgical Rehabilitation
If surgery is required, your STAR Physical Therapy rehabilitation program will have some additional elements. You may need to use crutches for several days after surgery. Many patients are able to bear some weight on their foot within the first week. A protective dressing will cover your incisions, and the stitches are usually removed within 10 to 14 days (unless they are absorbable stitches, which will not need to be taken out).
Our physical therapists will help you recover and gradually return to your normal activity level. We may recommend the use of a stationary bike within 10 to 14 days of your surgery. If you are a runner, our physical therapy program may enable you to begin a light jogging program within six weeks and resume full activity within eight to 10 weeks, although the time required for recovery and rehabilitation varies for each individual.
STAR Physical Therapy provides physical therapy in Fairport and Rochester.
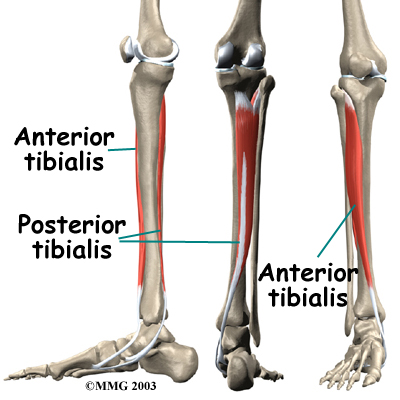
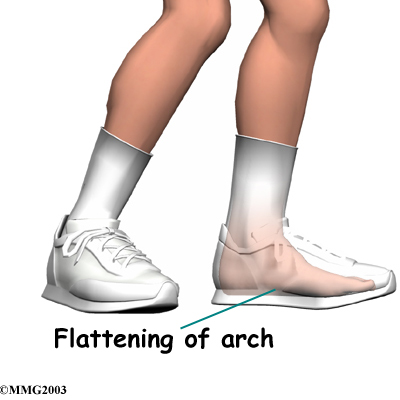 Posterior shin splints are generally caused by imbalances in the leg and foot. Muscle imbalances from tight calf muscles can cause this condition. Imbalances in foot alignment, such as having
Posterior shin splints are generally caused by imbalances in the leg and foot. Muscle imbalances from tight calf muscles can cause this condition. Imbalances in foot alignment, such as having 
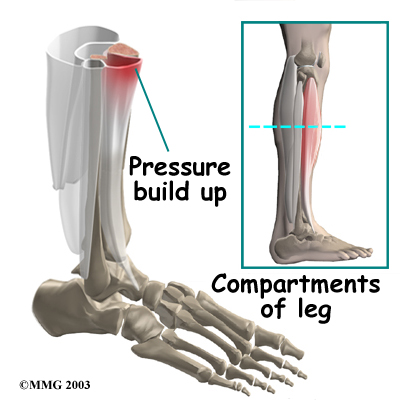
 If compartment syndrome is discovered and diagnostic tests show high pressures within the tissues of the lower leg, surgery may be recommended right away. The procedure to remove the pressure is called fasciotomy. Fascia is the connective tissue around and between muscles and organs. The surgeon makes a few
If compartment syndrome is discovered and diagnostic tests show high pressures within the tissues of the lower leg, surgery may be recommended right away. The procedure to remove the pressure is called fasciotomy. Fascia is the connective tissue around and between muscles and organs. The surgeon makes a few